In a new study from LVPEI, Drs. Bhupesh Bagga, Gowtham Lakshminarayanan, and others report on the outcomes of photodynamic antimicrobial therapy with Rose Bengal as an adjuvant treatment in patients with Acanthamoeba keratitis.
The cornea, the transparent front dome, is the eye’s first line of defense against the outside world. Occasionally, the cornea is infected by pathogens, such as bacteria, fungi, or viruses, after some form of trauma (a blade of grass, say). Acanthamoeba, a genus of soil- and water-dwelling amoeba, can also infect the cornea, causing a sight-threatening inflammation known as Acanthamoeba keratitis (AK). Exposure of the eyes to contaminated water, such as in agricultural fields or washing contact lenses with tap water, is the most common cause of this disease. An estimated 30-40% of AK patients require corneal transplantation (keratoplasty). Even after that, many patients do not regain good visual acuity and require additional surgery. Non-surgical treatments like topical biguanides come with the risk of corneal scarring, while miltefosine—an anti-parasitic drug—has shown promise but is still under testing. The issues raise the need for more treatment options.
Photodynamic therapy (PDAT) is an antimicrobial treatment that uses a chemical photosensitizer and a light source (e.g., a laser). PDAT’s effectiveness depends on the photosensitizer, a light-sensitive compound that, when exposed to light, generates reactive oxygen species that are lethal to microbial cells. Rose Bengal, a reddish-pink dye used in ocular surface diagnosis, has shown promise as an effective photosensitizer. One case series showed that PDAT with Rose Bengal (PDAT-RB) reduced the need for keratoplasty in 72% of patients with bacterial keratitis. Could the treatment also be used against Acanthamoeba, especially in the early stages of infection?
In a new study published in the Journal of Ophthalmic Inflammation and Infection, Drs. Bhupesh Bagga, Gowtham Lakshminarayanan, and others from LVPEI present the outcomes of PDAT-RB as an adjuvant treatment in patients with Acanthamoeba keratitis. The study included 14 patients with AK who were primarily treated using a combination of topical biguanides and chlorhexidine, a broad-spectrum antimicrobial drug. In addition to the primary treatment, the patients also underwent PDAT twice a week, using 0.1% Rose Bengal as the photosensitizer.
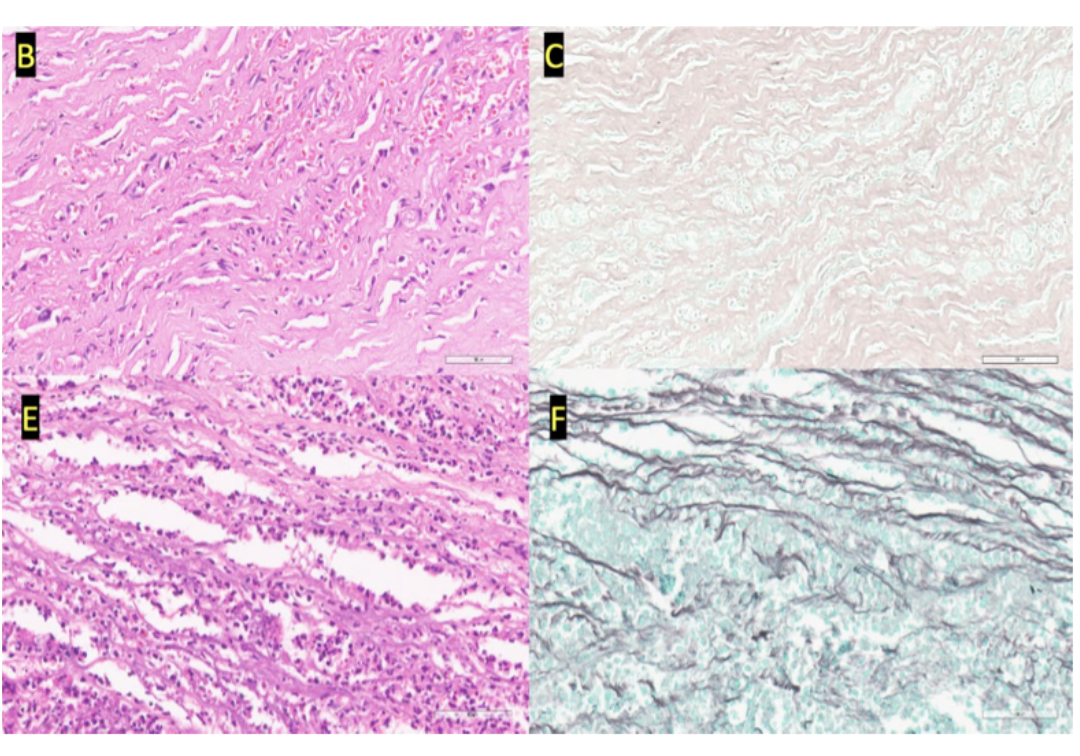
Patients with keratitis display a collection of inflammatory cells, called ‘infiltrate,’ which make the cornea opaque. Before treatment, all patients had infiltrates bigger than 8 mm in diameter (along both meridians) and deeper than 300 microns. Primary treatment with PDAT-RB reduced the average diameter to 5.7 mm (vertical) and 5.9 mm (horizontal), and the median depth to 250 microns, indicating reduced inflammation. The infection was resolved in 85.7% of patients within 67-150 days. Only two patients had to undergo a transplant. On average, the visual acuity of patients improved from total blindness (2.52 logMAR), even though they continued to have severe vision loss (1.6 logMAR). The study shows that Rose Bengal is an effective photosensitizer and that early intervention with PDAT-RB can yield promising results in Acanthamoeba keratitis.
'PDAT-RB–induced reactive oxygen species and free radicals may serve as powerful agents in eliminating Acanthamoeba from infected eyes,' says Dr. Gowtham Lakshminarayan, Research Assistant Scientist at the Dr. Chigurupati Nageswara Rao Ocular Pharmacology Research Centre, LVPEI.
Citation
Bagga, B., Gowtham, L., Ahirwar, L. K., Sen, D., Jakati, S., Ali, M. H., & Sharma, S. (2025). Outcome of photodynamic therapy with Rose Bengal in conjunction with topical PHMB and chlorhexidine combination in Acanthamoeba keratitis. Journal of Ophthalmic Inflammation and Infection, 15(1), 18. https://doi.org/10.1186/s12348-025-00466-w
Photo credit: Fig. 3, Bagga et al.