Persistence Vs Aggression
Written by Soujanya Padikkal
Published 26th March 2026 / Last updated 30th March 2026
In a new study, researchers from LVPEI, Cole Eye Institute, Cleveland, and ABO Eye Institute report that in a form of ocular tuberculosis persistent inflammation after treatment is driven by the body’s immune system rather than the infection itself.
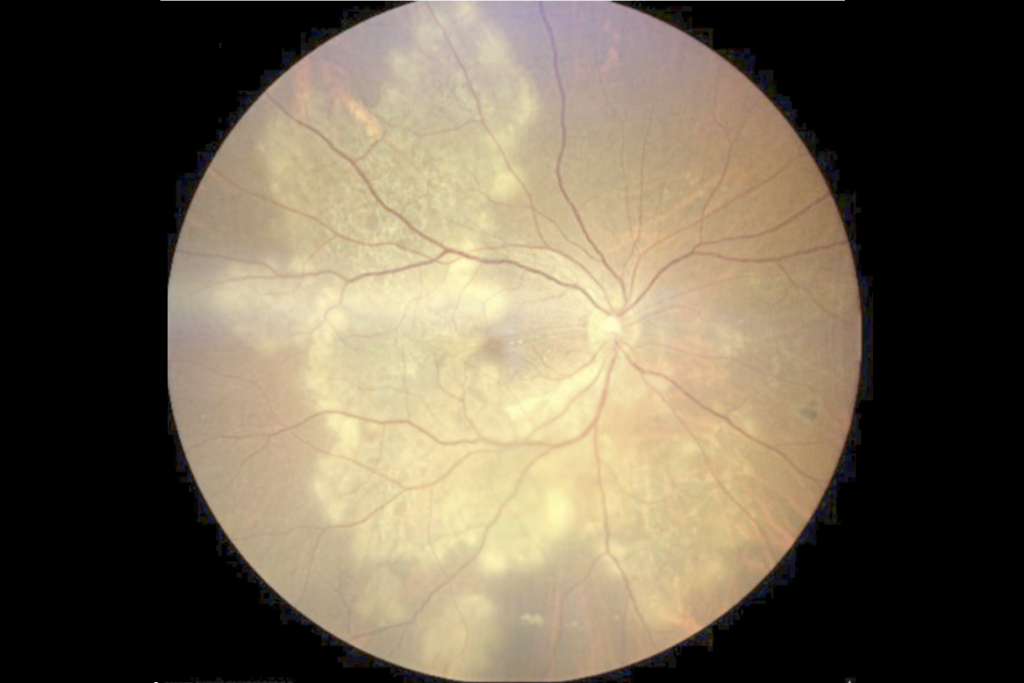
Photo credit: Figure 1.A, Kesav et al
Tuberculosis, the world’s top cause of bacterial infection deaths, primarily affects the lungs. The mycobacteria can then follow the bloodstream to infect other organs like the eye [1]. Ocular tuberculosis can manifest as tubercular serpiginous-like choroiditis (TB-SLC), where ‘snake-like’ lesions spread across the inner membranes of the eye. TB-SLC affects the choroid (the vascular layer that nourishes the retina), gradually damaging the retina and impairing vision. TB treatment involves a prolonged course of antitubercular therapy (ATT) where a combination of antibiotics is given over a period of 6 to 9 months to fight the infection. In addition, corticosteroids are prescribed to control immune-driven inflammation. However, a substantial number of patients continue to show inflammation markers even after the therapy ends.
What drives this inflammation remains unclear. There are two possibilities: either the infection is still present, or something else is triggering the body’s immune response even after the bacteria have been cleared. Poor outcomes in TB-SLC are classified into two types: ‘paradoxical worsening,’ which occurs within the first two to four weeks of starting ATT; and ‘persistent inflammation’ that occurs at the end of the treatment in about 10-15% of TB-SLC patients. Paradoxical worsening is relatively well understood while persistent inflammation remains under-researched. Clinicians lack a framework to identify which patients require monitoring or a different approach when the treatment does not work.
In a new study published in Translational Vision Science and Technology, Natasha Kesav, Shabtab Nasir and colleagues from LVPEI examine this gap. They analyzed data from 65 patients (46 male) with TB-SLC who had completed at least six months of the treatment. The study tracked disease activity using fundus autofluorescence — an imaging technique that distinguishes active from healed lesions. They used a scoring system called Total Immunosuppressive Load (TIL) to understand treatment intensity. TIL combines different forms of immunosuppressive therapies into a single score per visit, allowing them to compare how aggressively inflammation was treated across patients. They then used statistical modeling and network analysis to identify which factors were linked to persistent inflammation.
The study found that 12 patients (18.5%) had persistent inflammation at the end of the treatment, and two factors were associated with this outcome. Patients who received less aggressive corticosteroids in the first month of ATT were significantly more likely to have persistent inflammation at the end, indicating that the early anti-inflammatory therapy is critical. Interestingly, all 12 patients who had persistent inflammation at the end had already shown signs of it at the 3-month follow-up, making it an important timeline for clinicians. It was also noted that 15 of 17 affected eyes resolved with anti-inflammatory therapy without any change to the antibiotic regimen. Despite a cleared infection, the legacy of early immune dysregulation established by inadequate anti-inflammatory therapy seems to be driving late inflammation in a sub-set of patients with TB-SLC.
“When an infectious disease persists after prolonged antimicrobial therapy, it is quite a challenge for the clinician. Our study demonstrates that factors beyond infection could also be driving late persistence of inflammation is TB-SLC”, comments Dr. Soumyava Basu, Head, Uveitis Services, LVPEI and corresponding author of the paper.
Citation
Kesav N, Nasir S, Ali MH, Sawal RT, Narula R, Tyagi M, Basu S. Persistent Inflammation After Anti-Tubercular Therapy in Tubercular Serpiginous-Like Choroiditis: A Multivariate and Network-Based Risk Analysis. Transl Vis Sci Technol. 2025 Dec 1;14(12):27. doi: 10.1167/tvst.14.12.27. PMID: 41533872; PMCID: PMC12758418.
[1] While tuberculosis infects the lungs, some 20% of TB infections develop in the lymph nodes, brain, gut, eyes, or other organs. Read more here: https://www.thehindu.com/opinion/op-ed/the-challenge-of-extra-pulmonary-tb/article68174298.ece